We are writing about this now because a recent AWS piece on radiology workflows puts its finger on an issue that is still underestimated.
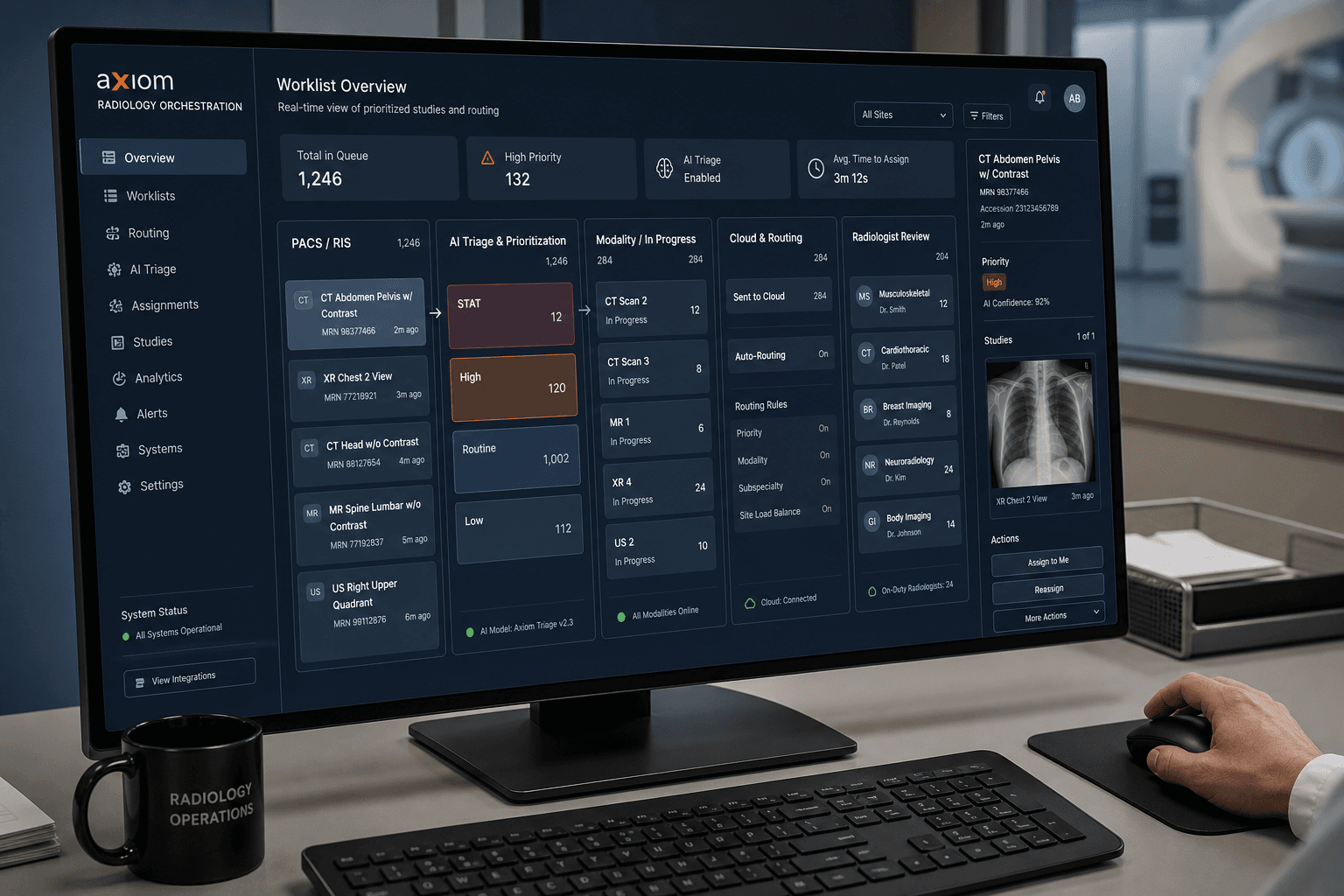
What makes it useful is not that it adds one more medical-AI demo to the pile. It starts from a very concrete operating problem: how studies get prioritized, contextualized, assigned, and reviewed before they become reports.
When people talk about radiology AI, they often jump first to report generation.
That is easy to understand: it is simple to show, close to the final deliverable, and it makes the machine look like it is doing part of the radiologist's job.
Report generation is also overrepresented because it is easier to automate partially and to evaluate in a relatively deterministic way.
But radiology AI obviously does not stop at reporting. It also includes diagnosis support, pathology detection, triage, prioritization, and integration into the clinical workflow.
But if you look at radiology as an operating system rather than as a sequence of isolated model outputs, the real bottleneck usually appears elsewhere.
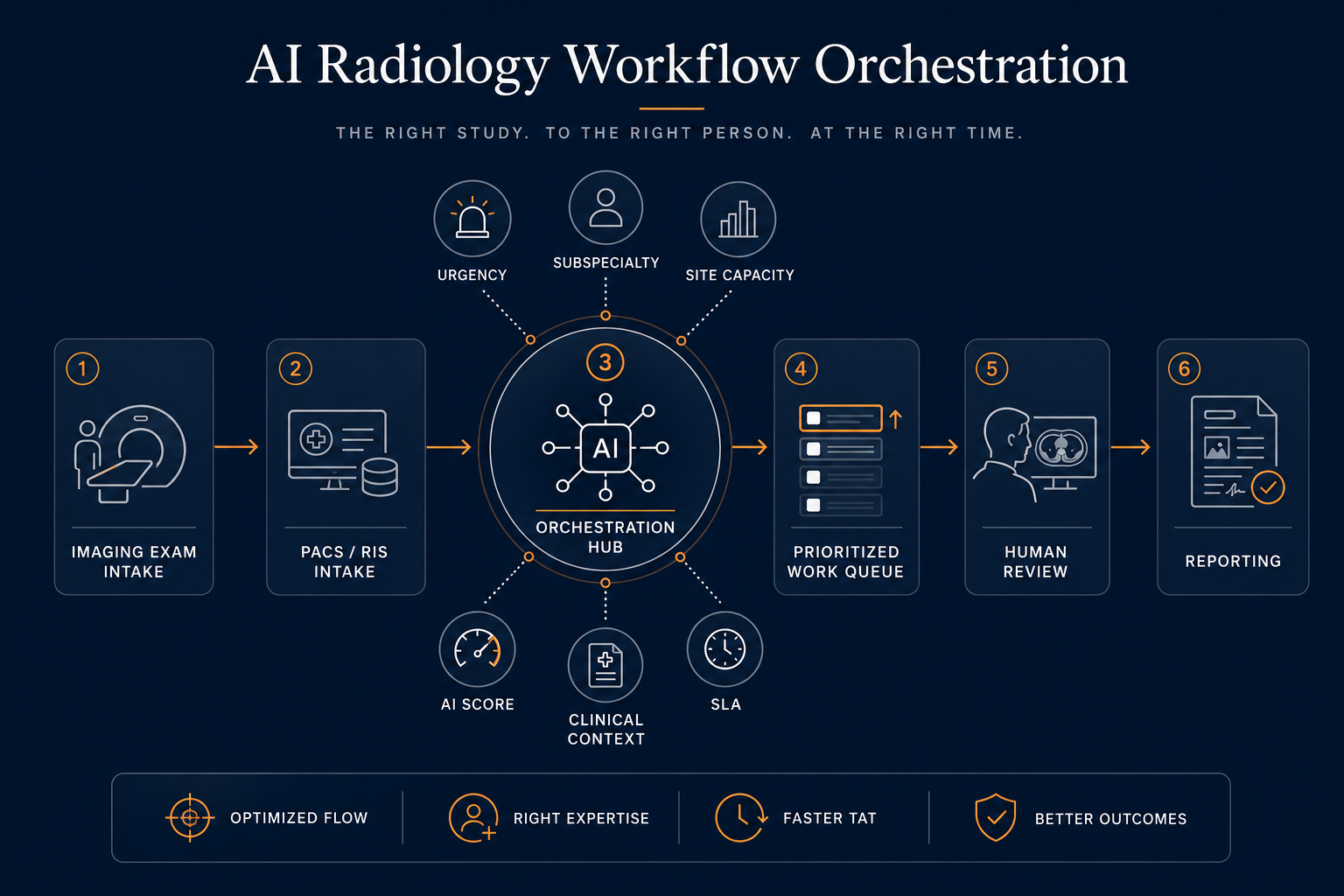
The highest-leverage AI layer is not only writing faster. It is routing the right study to the right radiologist or care team at the right time, with the right context, and under the right review loop.
That is the layer where orchestration, prioritization, human ownership, and systems integration matter more than one more polished report draft.
In my experience working on AI products in medical imaging, this gap between the demo and the real operational constraint shows up very quickly. The challenge is not only whether a model can detect or describe something. It is whether the result lands inside a workflow that clinicians can actually trust, adopt, and scale.
The wrong default debate
A lot of AI discussion still collapses the radiology workflow into one question: can the model help produce the report?
That question is not useless. Reporting is obviously part of the chain. But it is a narrow slice of the problem.
A review published in the Journal of the American College of Radiology framed AI workflow applications much more broadly, spanning the imaging pathway from test ordering and scheduling to worklist management, interpretation, and report communication. That is already a strong clue that the biggest economic and operational gains may not sit in dictation alone.
AWS makes the same point from a systems angle in its post on intelligent radiology workflow optimization with AI agents. Their argument is straightforward: traditional worklists still rely on rigid rules and often fail to account for radiologist specialization, workload, fatigue, and case complexity. In practice, that means suboptimal assignment, delays, and queue behavior that does not reflect clinical reality.
That source is especially useful because it is concrete about the workflow problem, but it should still be read with the right level of caution. It is an AWS-authored piece illustrating a possible architecture: a credible operator frame and a plausible design pattern, not neutral production-outcome evidence from a deployed customer.
That is the part many AI conversations still underweight.
Radiology is not just a reading task. It is a flow-management problem.
Where time is actually lost, before the report
One reason the report-generation narrative is incomplete is that a meaningful share of friction happens before a radiologist starts dictating.
First, the study has to reach the right practitioner at the right moment.
Then they often need the right context: priors, clinical history, relevant notes, and the right urgency signals. AWS also addressed this in a separate post on accelerating radiology imaging workflows with relevant clinical context, arguing that radiologists still spend non-trivial time manually gathering relevant documents and prior exams.
That sounds mundane, but operationally it matters a lot. If context retrieval is fragmented, the reading step is slower and the clinical decision is less fluid.
There is also the issue of interruptions and task switching.
A study in Academic Radiology on radiology workflow dynamics found that separating image-interpretive from non-image-interpretive workflow improved perceived disruptions, workload, workplace satisfaction, and consult quality. That finding matters because it reminds us that the reporting act is embedded inside a noisy environment full of interruptions, consults, prioritization decisions, and non-reading tasks.
So when someone says, “AI will transform radiology because it can help draft the report,” my first reaction is: maybe. But that is often not where the queue is breaking.
The stronger proof points are in prioritization and queue management
If you look for the clearest evidence of workflow value, the most convincing examples are not usually about prose generation. They are about triage, prioritization, and time to action.
A study in European Radiology on AI-based chest X-ray worklist prioritization reported a substantial reduction in average report turnaround time for critical findings such as pneumothorax versus a simple FIFO workflow. The study is also useful because it includes an important caveat: prioritization systems need safeguards against starvation and unsafe false negatives. In other words, orchestration matters, but orchestration also needs policy.
A second strong example comes from Radiology: Cardiothoracic Imaging, where an AI tool for incidental pulmonary embolism detection and worklist prioritization dramatically reduced time to diagnosis and notification compared with routine workflow, while also reducing missed cases. That is a very different kind of value proposition from “the model can write text.” It is about whether the system helps the right case surface fast enough to change care.
A 2024 European Radiology paper on AI triaging of outpatient chest radiographs is also interesting because it supports a workload-management thesis: AI triage could reduce the effective review burden while maintaining noninferior sensitivity in a simulated setting.
They point to the same conclusion: the economic and clinical leverage often sits in queue design, routing, prioritization, and escalation logic.
Why orchestration becomes the real product layer
Once you accept that the bottleneck is not only writing, the architecture discussion changes.
The product is no longer just “a model that detects X” or “a copilot that drafts Y.”
The product becomes a workflow layer that must answer questions such as:
- Which study should be read first?
- Which findings should change priority?
- Which radiologist or subspecialist should receive the case?
- Which priors and clinical documents should be surfaced automatically?
- How is AI output presented and reviewed inside the native workstation?
- What happens when the model is uncertain, late, or wrong?
This is why standards and integration matter so much. The SIIM/IHE AI Workflow for Imaging technical framework is a useful reminder that this is not a cosmetic layer. Workflow orchestration is serious enough to require infrastructure-level thinking.
The same logic appears in enterprise imaging architectures on AWS. Their post on improving medical imaging workflows with AWS HealthImaging and SageMaker is not just a model story. It is an integration story: imaging systems, storage, inference, review, and downstream actions all have to cooperate.
That is the part that decides whether a radiology AI product remains a demo or becomes an operational tool.
What my Gleamer experience made obvious very early
Part of why this topic resonates with me is that, from my own time at Gleamer, I saw how fast medical AI moves beyond debates centered on scores, benchmarks, and model quality alone.
You stop debating only model quality and start dealing with harder realities:
- cloud versus on-premise deployment constraints
- integration into existing radiology software environments
- latency expectations inside clinical workflows
- productization across heterogeneous partner setups
- review, acceptance, and ownership of AI outputs
That is one reason I am skeptical whenever radiology AI is discussed as if it were mainly a text-generation problem.
In my experience, the hard part was much more often adapting architecture and workflow to real environments. It is not only a model or performance issue: multiple personas interact with these systems, or depend on them indirectly — radiologists, technologists, IT leads, product teams, technical partners, integrators, and sometimes hospital management. The real challenge is making the system useful, understandable, and controllable across that whole chain, with different constraints depending on the deployment context.
That public positioning is also visible in Gleamer's current product language. On Gleamer Copilot and GleamerOS, the company emphasizes worklist prioritization, RIS/workstation integration, "shadow mode," and reviewable AI outputs rather than only raw detection performance. That is a more mature framing of workflow AI.
Even the clinical evidence that is easiest to cite publicly tends to reinforce an assistive workflow story, not a replacement story. Gleamer's published materials around fracture and chest X-ray assistance highlight gains in sensitivity and, in some studies, reading efficiency. Useful signals, yes. But still within a human-led operating loop.
That is the right framing.
Human in the loop is not a weakness of the product
A recurring mistake in AI marketing is to treat human review as a temporary compromise, as if the ideal system would remove it once the models are good enough.
Human review is not just there because regulation exists or because the model is imperfect. It is there because the workflow itself needs a clear accountability layer.
You can see that operationally in several vendor approaches.
Blackford Platform explicitly presents an accept/reject review step before AI results are sent into PACS. Gleamer's public "shadow mode" framing also points in the same direction: AI should be visible, reviewable, and rejectable inside the clinician's native workflow. Aidoc's radiology workflow positioning likewise emphasizes unified review inside existing worklists rather than disconnected model outputs.
This is an important design lesson far beyond radiology.
The mature AI product is often not the one that tries to hide the human. It is the one that makes the handoff between machine recommendation and human ownership operationally clean.
The right questions to evaluate an AI solution
If I were evaluating radiology AI products today, I would spend less time on the most polished report-generation demo and more time on the workflow contract.
I would ask:
- Assignment logic: how does the system route studies across subspecialties, sites, urgency levels, and current reader capacity?
- Prioritization safety: how does it prevent unsafe starvation, queue distortion, or overconfidence on false negatives?
- Context retrieval: does it surface the right priors and clinical documents automatically, or is that still manual?
- Human review: where can the radiologist inspect, accept, reject, or override the AI result?
- Integration depth: how does it integrate with PACS, RIS, EHR, cloud, and on-premise infrastructure?
- Deployment reality: what changes between a controlled demo environment and a heterogeneous hospital or partner deployment?
- Observability: can you measure turnaround, escalations, review behavior, and operational impact beyond model metrics?
Those questions are much closer to actual value capture.
The durable advantage is operable orchestration
I do not think report generation is irrelevant.
I do think it is often overrated relative to the harder, more structural workflow layer around it.
In radiology, the durable advantage is not only whether a model can produce acceptable text faster.
It is whether the system can:
- triage intelligently
- route safely
- surface context automatically
- fit inside existing clinical environments
- preserve clear human ownership
- and improve the real queue rather than just the visible output
That is where AI becomes infrastructure instead of theater.
And that is why, in radiology, the real bottleneck is usually not report generation.
It is work assignment.
Verified sources
Verified on 2026-05-22.
Primary workflow sources
- AWS — Intelligent radiology workflow optimization with AI agents
- AWS — Accelerating radiology imaging workflows with relevant clinical context on AWS
- AWS — Improving medical imaging workflows with AWS HealthImaging and SageMaker
- JACR — Workflow Applications of Artificial Intelligence in Radiology and an Overview of Available Tools
- SIIM/IHE — AI Workflow for Imaging Technical Framework Supplement
Quantitative workflow evidence
- European Radiology — Smart chest X-ray worklist prioritization using artificial intelligence software: a clinical workflow simulation
- Radiology: Cardiothoracic Imaging — AI Tool for Detection and Worklist Prioritization Reduces Time to Diagnosis of Incidental Pulmonary Embolism at CT
- European Radiology — Use of artificial intelligence in triaging of chest radiographs to reduce radiologists’ workload
- Academic Radiology — Radiology Workflow Dynamics: Effect of Change From the Traditional Reading Room Model to an Image Interpretation Center on Disruptions, Reading Times, and Report Quality
Supporting product and deployment sources
- Gleamer Copilot
- GleamerOS
- Gleamer — A prospective approach to integration of AI fracture detection software in radiographs into clinical workflow
- Gleamer — Artificial intelligence and pelvic fracture diagnosis on X-rays: a preliminary study on performance, workflow integration and radiologists’ feedback assessment
- Blackford Platform
- Aidoc — Radiology AI operating system
Interpretive conclusions in this article are my own. Publicly attributed facts are limited to the sources above, and my Gleamer-related operational observations are framed as personal experience rather than independent public claims.